AUCTORES
Globalize your Research

review | DOI: https://doi.org/10.31579/2693-4779/31
1* North Manchester General Hospital, Delaunays Road Crumpsall Manchester, M8 5RB, United Kingdom
2 Salford Primary Care Trust (EPIC Extended Primary Integrated Care), City Approach Eccles, Salford, Manchester, Lancashire, M30 OBL United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo. North Manchester General Hospital, Department Of Urology, Delaunays Road, Manchester, M8 5RB. United Kingdom.
Citation: Anthony K-G Venyo, O Adaramodu. (2021) Salmonella Breast Abscess and Salmonella Mastitis: A Review and Update of the Literature. Clinical Research and Clinical Trials. 3(2); DOI:10.31579/2693-4779/031
Copyright: © 2021 Anthony Kodzo-Grey Venyo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 March 2021 | Accepted: 05 April 2021 | Published: 08 April 2021
Keywords: salmonella breast abscess; salmonella mastitis; bacteriology culture; widal tests, stool culture; blood culture; aspiration; incision and drainage; mastectomy; unilateral; bilateral; recurrence; non-lactating; females; males; children; infants
Salmonella breast abscess / mastitis is a rare infection which can affect children and adults. It can affect females more commonly who are non-lactating and it does affect males as well as individuals who have predisposed conditions including: the immunocompromised, diabetics, rheumatoid arthritis, malignancies and other diseases. It may be acute, chronic, unilateral, or bi-lateral, as well as it may be recurrent if it is not appropriately treated. There tends to be a history of previous enteric fever (abdominal pain, vomiting, diarrhoea) which may not have been treated or adequately treated but this history has tended not to be apparent at the time of presentation. Manifestations of the disease tend to include a short- or long-history of: lump/mass in the breast which may or may not be painful, a history of previous diarrhoea, weight. The breast examination findings tend to be non-specific with some the findings including tenderness or no tenderness, a mass that may or may not be tender, a fluctuant lump that may feel like containing fluid, a firm or hard feeling lump that may mimic carcinoma of the breast. Confirmation of the diagnosis tends to be via obtaining culture and sensitivity results of a Salmonella organism and its sensitivity pattern. Treatments that have been given include: Utilization of correct antibiotics based upon the sensitivity pattern of the cultured organism, plus surgical treatment which could be complete aspiration of the pus, incision and drainage of the abscess or in cases where carcinoma of the breast was the provisional diagnosis or the diagnosis is unknown subcutaneous mastectomy and this can be avoided by biopsy of a lesion that mimics a malignant lesion. Follow up of patients is required to ensure the breast lesion has fully resolved. Adoption of the World Health organization guidelines for the prevention of Salmonella infection would help avoid the development of the infection. Urine culture, routine haematology and biochemistry blood tests as well as serology WIDAL tests and stool culture are some of the tests that tend to be undertaken in the investigation of the disease and in order to diagnose the disease a good history would be required including a history of travel from a non-typhoid endemic area to an endemic area.
Conclusions: Salmonella breast abscess / mastitis is an uncommon disease which clinicians should have a high index of suspicion for. A history of previous enteric fever does help in suspecting the disease which at times does need to be distinguished from carcinoma of the breast. The diagnosis is confirmed by obtaining the culture results of the pus from the breast abscess / breast tissue. If all breast lesions are biopsied especially in cases of suspicion of a breast cancer and a past history of abdominal pain, diarrhoea and vomiting the results of the pathology examination of the specimen would negate malignancy and confirm an infection which would help in avoiding mastectomy procedures and enable utilization of antibiotics and drainage/aspiration of abscess to provide adequate treatment.
It has been iterated that Staphylococcus aureus is the commonest cause of breast abscess. [1], and additionally, streptococci, gram-negative bacilli, as well as anaerobes could cause breast abscess. [2, 3, 4, 5] Breast abscess that is caused by Salmonella is said to be rare and it tends to occur as a late complication of enteric fever. [1, 6] it has been documented that breast abscesses had been reported to ensue Salmonella enterica serotype Typhi and para-typhi infections. [1] Furthermore, the development of breast abscesses that had been related to non-typhoidal Salmonella are very rare. [2, 7] Because of global travelling, cases of Salmonella mastitis and breast abscess can be encountered anywhere in the world. Nevertheless, because of the rarity of Salmonella infections of the world, it would be envisaged that majority of clinicians globally would not be familiar with the manifestations of the infection. All clinicians need to be familiar with the manifestations, investigation and diagnosis of the commonest type of Salmonella infection in order to have an understanding of the biological behaviour of Salmonella mastitis and Salmonella breast abscess. Additionally, in order that clinicians globally are reminded to have a high-index of suspicion of Salmonella mastitis and Salmonella breast abscess it would be important to provide a review of the literature on the disease entity. The ensuing article on Salmonella mastitis and Salmonella breast abscess is divided into two parts including: (A) Overview which has discussed various aspects of Salmonella infection generally and (B) Miscellaneous narrations and discussions from some case reports, case series, and studies related to Salmonella mastitis and Salmonella breast abscess.
To review and update the literature on Salmonella mastitis and Salmonella breast abscess.
Various internet data bases were searched including: Google, Google Scholar, Yahoo and PUB MED. The search words that were used included: Salmonella breast abscess, Salmonella mastitis. Twenty nine references were identified which were used to write the review and update of the literature on Salmonella Mastitis and Salmonella breast abscess which has been divided into two parts: (A) Overview which has discussed general aspects of Salmonella infection including Salmonella infections of the bowel and (B) Miscellaneous narrations and discussions related to some case reports, case series, and studies related to Salmonella mastitis and Salmonella breast abscess.
[A] Overview / general statements
Essential features of Salmonella infection
Some of the summations related to the epidemiology of Salmonellosis have been documented as follows: [8]
With regard to sites of infection of Salmonella, it has been iterated that Salmonella typhi could infect the entire gastrointestinal tract; nevertheless, Salmonella infection tends to be typically found within the terminal ileum, appendix, and ascending colon and that non-typhoidal Salmonella does infect the small and large bowel.
Salmonella typhi is said to typically spread to the liver, spleen, bone marrow, and lymph nodes [8].
It has been iterated that extra-intestinal spread of Salmonella tends to be uncommon in non-typhoidal Salmonellosis but this could occur with regard to severe Salmonellosis [8].
Generally it would be stated that with regard to human beings Salmonella infection does tend to be reported sporadically in almost every organ of the body including: the penis, scrotum, epididymis and testis, urinary bladder as well as the urinary tract organs, the genital tract organs including the ovaries, fallopian tubes, and the uterus, the lungs, the heart, the bones, the brain as well as the breast. Because Salmonella infection only tends to affect the breast on very rare occasions, it would be envisaged that majority of clinicians with the developing countries as well as the developed countries would never have encountered a case before and they would also tend not to be familiar with the manifestations, clinical examination findings and the diagnostic features as well as management of Salmonella infections of these rare sites.
With regard to the pathophysiology of Salmonellosis, it has been iterated that Salmonella does possess cellular mechanisms that enable bacterial proteins to be transferred to enterocytes as well as M cells with the subsequent growth within endosomes [8].
It has also been iterated that subsequent events do include an inflammatory response with neutrophil recruitment as well as mucosal damage [8].
It has been documented that the host immune response does typically control non-typhoidal infection; nevertheless, the very young individuals, elderly individuals, debilitated as well as immunosuppressed individuals could lack the response that is necessary to control the infection [8].
It has been iterated that Salmonella typhi do more commonly invade M Cells [8].
It has also been stated that Salmonella bacteria tend to be phagocytosed by histiocytes within underlying lymphoid tissue [8].
It has furthermore been stated that the Salmonella bacteria do proliferate and disseminate widely through blood vessels as well as lymphatic channels [8].
The ensuing summations have been made regarding the aetiology of Salmonellosis: [8]
Salmonella are known to be gram negative bacilli [8].
Salmonella typhi tends to be found in human beings [8]
Non-typhoidal species tend to be found in human beings, domestic animals as well as wild animals [8].
It has been iterated that generally, Salmonella infection does occur via ingestion of Salmonella contaminated food or water or via the faecal-oral route [8].
It has also been stated that Non-typhoidal Salmonella tend to be commonly encountered in food as well as companion animals with the inclusion of poultry, cattle, swine, parrots, cats, dogs, as well as turtles [8].
It has also been documented that eggs, milk, meat, poultry, as well as contaminated vegetables have commonly been implicated in Salmonellosis [8].
It has been iterated that direct person to person transmission of Salmonella infection from pets could occur and in this setting, the source of the transmission of Salmonellosis might not appear to be ill or may be symptomless [8].
Symptoms of non-typhoidal Salmonellosis affecting the bowel:
The symptoms of non-typhoidal Salmonellosis of the bowel have been stated to generally commence 12 hours to 36 hours pursuant to ingestion of the Salmonella bacteria but this could commence pursuant to from between 6 hours and 72 hours [8].
Ingestion of very few Salmonella bacteria could cause Salmonellosis [8].
It has been iterated that typically individuals who are afflicted by non-typhoidal Salmonella infection of the bowel do tend to suffer self-limited illness that tend to manifest with diarrhoea, abdominal pain, fever, nausea, and on rare occasionally vomiting which tends to be unpleasant but this tends to be rarely life threatening [8]
It has been iterated that non-typhoidal infection of the bowel could be life threatening with regard to infants, the elderly, the immunocompromised, and debilitated patients, as a result of dehydration or dissemination of the non-typhoidal bacteria [8].
It has also been iterated that on very rare occasions, toxic megacolon could complicate the non-typhoidal Salmonellosis of the bowel [8].
It has been documented that individuals who have achlorhydria or hypochlorhydria from medications, chronic Helicobacter pylori infection or from other causes are at a higher risk for the development of non-typhoidal Salmonella infection [8].
It has been pointed out that some individuals do develop a reactive arthritis which could last for months as well as lead to chronic arthritis [8].
Symptoms of typhoid enteritis fever
It has been iterated that typhoid fever affecting the bowel does cause symptoms shortly after ingestion of the salmonella bacteria [8].
It has been documented that individuals who are afflicted by Typhoid Salmonella infection of the bowel tend to suffer from severe abdominal pain, bloody diarrhoea, bloating of abdomen, nausea, vomiting, as well as head ache [8].
With regard to Salmonella typhoid fever infections of the bowel tends to be associated with a brief asymptomatic period that is ensued by bacteraemia with fever as well as flu-like illness [8].
It has stated that during the period of fever blood cultures tend almost always to be positive for Salmonella typhi as well as antibiotic treatment could be lifesaving at this stage [8].
It has additionally been iterated that with progression of the salmonella typhi disease in untreated patients, the development of high fever and abdominal pain does occur which could simulate appendicitis and this could last for about two weeks [8].
It has been pointed out that when patients survive from the typhoid enteric fever, their symptoms slowly abate [8].
It has been documented that possible extra-intestinal complications of Salmonella typhi disease of the bowel do include: central nervous disease, endocarditis, myocarditis, pneumonia, cholecystitis, as well as osteomyelitis and that patients who have Sickle cell disease tend to be particularly prone to the development of osteomyelitis [8].
It has been pointed out that relapses of Salmonella typhoid disease could occur [8].
Diagnosis of Salmonella infection of the bowel.
The diagnosis of Salmonella infections of the bowel have been summated as follows: [8]
It has been pointed out that Non-typhoidal Salmonellosis has traditionally been diagnosed based upon the undertaking of stool culture even though many individual patients do not tend to seek any medical attention [8].
It has been iterated that recently a PCR based assay had been introduced and this in addition to Salmonella species bacteria, also does detect Campylobacter group, Shigella species, Vibrio group, Yersinia enterocolitica, Shiga toxin 1 and 2, Norovirus G1 / GII, Rotavirus A and Aeromonas species [8].
It has also been stated that serotyping tends to be undertaken to characterize outbreaks of the disease [8].
It has additionally been iterated that typhoid fever tends to be diagnosed by means of blood culture or stool culture [8].
It has been pointed out that within the developing countries of the world where laboratory facilities might not be available readily, the disease has tended to be treated empirically [8].
Factors of Prognostication in Cases of Salmonella of the bowel [8]
Non-typhoidal salmonellosis of the bowel [8]
It has been iterated that non-typhoidal Salmonella infection of the bowel tends almost always to be a self-limited infection, with the exception of infants, the elderly, immunocompromised as well as debilitated patients
It has also been stated that antibiotic treatment usually tends to be effective in patients who have non-typhoidal disease of the bowel even though the development of resistance of the organism to antibiotics is a growing problem.
Typhoid fever (Salmonella typhoid infection of the bowel [8]
It has been stated that without treatment of Salmonella typhoid bowel disease, the outcome could be lethal even with regard to healthy patients but the prognosis of the disease tends to be worse in infants, elderly individuals, immunocompromised individuals, as well as debilitated patients.
It has been pointed out that prompt commencement of antibiotic treatment does greatly improve the outcome of patients, even though the development of antibiotic resistance has tended to be a growing global problem [8].
The treatment of Salmonella infections of the bowel have been summated as follows: [8]
It has been iterated that with regard to Salmonella typhi infections of the bowel, utilization of antibiotic treatment tends to be obligatory and antibiotic treatment should not be delayed in order to obtain confirmation of the laboratory test results [8].
Macroscopic gross examination features of the bowel in Salmonella infections of the bowel. [8]
Microscopy histopathology examination features of Salmonella infections of the bowel: [8]
Differential diagnosis of Salmonella infections of the bowel.
Salmonella of the breast is very uncommon.
The incidence of mastitis / breast abscess in patients who have typhoid has been stated to be 0.3% in 1930 by Close and Sebeng and 0.5% in 1937 by Peziski in a study of 1,196 cases of typhoid fever over a period of 2 years. [9]
With regard to females, the incidence of Salmonella infection of the mammary gland was 0.90% [9] [10] [11] [12] Razeq and associates [13] and Edelstein [2] had isolated Salmonella Landwasser and Serogroup B in breast abscess respectively.
Salmonella infection of the breast could be:
Acute
Chronic
Unilateral
Bilateral
Salmonella mastitis / abscess can be seen in:
The female
The male on rarer occasions
Salmonella mastitis / abscess may be found in the following:
A healthy individual who has no history of any significant co-morbidity
An individual who is known to have diabetes mellitus
Immunocompromised individual
An individual who has had a history of salmonella infection of the bowel recently or many months earlier that usually had not been treated. There may not be a definite history of previous diarrhoea or salmonella mastitis / abscess at the time of presentation of the disease but when the diagnosis of Salmonella infection of the breast has been established based upon microbiology culture of Salmonella organism from the aspirate of the breast abscess or breast specimen, a review of the past medical history of the patients tends to reveal a past history of diarrhoea / diagnosis of previous Salmonella infection that had not been treated.
Cases of salmonella infection of the breast could be found in some individuals who have rheumatoid arthritis or fibroadenoma of the breast.
With regard to ladies who have Salmonella mastitis / abscess these usually tend to occur in non-lactating women in comparison with staphylococcus mastitis / breast abscess which tends to occur in lactating women. Salmonella infection of the breast can also affect children and infants.
Salmonella mastitis / breast abscess could be due to Salmonella typhi or salmonella para-typhi infection.
The presentation of salmonella infection of the breast in the form of mastitis or breast abscess does vary from one individual to another and the presentation tends to be non-specific and does simulate the presentation of various breast conditions but generally Salmonella infection of the present could manifest as follows:
Lump / Mass - The finding of a lump/mass within the breast of a few days duration or the breast lump could be present over a long-period of time.
Discomfort / Pain in breast - The lump / mass in the breast may be associated with mild discomfort or pain.
No nipple discharge - There tends not to be any discharge associated with the lump/mass
Nipple discharge - Few of the reported cases have been associated with discharge from the nipple but majority have not been associated with discharge.
Sex of patient – majority of patients who have been reported as having Salmonella mastitis / Salmonella breast abscess have tended to be female but salmonella infection / abscess of the breast has also been reported in males.
Age – Salmonella infection of the breast can affect individuals including children and adult.
Fever – some cases of Salmonella of the penis do not tend to be associated with fever but in some cases there may be an antecedent history of low-grade or high fever that may be antecedent or may exist contemporaneously with pain / lump / mass within the breast.
Vomiting – In some cases of Salmonella mastitis or Salmonella breast abscess there could be an antecedent history of gastroenteritis type of symptoms that include vomiting and on a number of occasions the patient who has had vomiting in the may not report a previous history of vomiting and often a history of previous vomiting may be obtained after the diagnosis of salmonella abscess / mastitis has been made in a retrospective history taking.
Diarrhoea – A number cases tend to be associated with a previous episode of loose stool or diarrhoea which may have settled and the individual patient may have forgotten about the diarrhoea; nevertheless, in other patients there could be contemporaneous episodes of diarrhoea.
Abdominal pain / discomfort – Some individuals may have a past history of abdominal pain / discomfort and occasionally there could be concurrent abdominal pain / discomfort that may tend to be associated with fever, vomiting / diarrhoea but is often not the case of some patients who would not report abdominal pain.
Some of the findings on clinical examination in cases of Salmonella breast abscess include the following:
Microbiology tests
Urine
Urinalysis, urine microscopy and culture are tests that tend to be undertaken as part of the general assessment of all individuals who have Salmonella mastitis or Salmonella breast abscess but the results would tend to be normal and if there is evidence of urinary tract infection this would be treated with appropriate antibiotics to help improve the general condition of the patients but the results would not be diagnostic of Salmonella abscess / of the breast or mastitis.
Stool
On the whole the results of stool culture in cases of Salmonella mastitis / breast abscess would tend to be negative for Salmonella infection but there could be a past history of a positive stool test result for Salmonella which the patient may have forgotten about but on rare occasions of the manifestation of the Salmonella breast abscess / mastitis being synchronous with an episode of Salmonella gastro-enteritis Salmonella could be isolated from the stool specimen but this is very rare.
Blood culture
Quite often during an episode of Salmonella breast abscess, blood cultures tend to be negative but in cases of a previously investigated Salmonella gastro-enteritis that was associated with bacteraemia, blood culture that is undertaken during the previous bacteraemia phase of the disease blood culture could yield a growth of Salmonella but this may not be remembered during the manifestation of Salmonella abscess of the breast and usually a retrospective review of the previous medical history of the patient could lead to the finding of positive Salmonella culture in the results of the patient’s past investigations.
Haematology blood test
In cases of Salmonella abscess of the breast / salmonella mastitis, the results of full blood count could be normal and on other occasions there is the possibility that the white blood cell count level could be raised but the results would not be diagnostic of Salmonella abscess / mastitis. Nevertheless, the results would tend to form part of the general assessment of all the patients.
Biochemistry blood tests
Routine biochemistry blood tests in cases of Salmonella breast abscess / mastitis tend to be normal but if there are diseases that affect the renal function or liver function test results these would be reflected in the results but the results themselves would not be diagnostic of Salmonella breast abscess or mastitis.
Widal test
Widal test is a serological test for enteric fever. Named after the inventor, Georges -Fernand Widal test is an indirect agglutination test for enteric fever or undulant fever and this test tends to be positive in cases of enteric fever. This test tends to form part of the assessment of patients who are suspected to have Salmonella breast abscess / mastitis but in a number of cases culture of the breast abscess would grow the Salmonella species but the Widal test which would be expected to be positive tends to yield a negative test result. This means that the finding of a negative Widal test does not mean that the breast abscess is not Salmonella abscess therefore it is important to send all specimens of the breast abscess for culture and sensitivity to confirm the result.
Radiology imaging
Chest X-ray
Chest X-ray tends to be undertaken at times when the lesion within the breast mimics a malignant lesion of the breast and this could form part of an initial screening in some parts of the world to ascertain if the individual has got metastatic lesion within the lungs but this has been superseded by CT scan of the thorax. However, in cases of Salmonella infection of the breast the chest x-ray would tend to be normal.
Mammography
Mammography has been undertaken in some cases of Salmonella breast abscess taking into consideration the suspicion of the lump/mass being a possible breast cancer but the features of the mammography would tend to demonstrate features that tend not to be suspicious of breast cancer.
Ultrasound scan
Ultrasound scan of the breast in cases of Salmonella abscess of the breast / mastitis tend to demonstrate the lesion within the breast and its echogenicity and most often does demonstrate the fluid nature of the breast lesion and based upon the fluid nature of the breast lump, aspiration / incision and drainage of the abscess can be undertaken as treatment as well as to submit the push for culture and sensitivity which would confirm the diagnosis.
Computed Tomography (CT) scan
Computed tomography scan of the breast / thorax would define the nature of the breast lesion which would tend to confirm non-contrast enhancing lesion as well as illustrate features that generally tend not to be suspicious of a malignant lesion within the breast. In cases that are suspicious for carcinoma of the breast based upon clinical examination CT scan of the thorax would tend to show normal findings within the lungs and thorax.
Magnetic Resonance Imaging (MRI Scan
Magnetic Resonance Imaging (MRI) scan of the breast / thorax would define the nature of the breast lesion which would tend to confirm non-contrast enhancing lesion as well as illustrate features that generally tend not to be suspicious of a malignant lesion within the breast. In cases that are suspicious for carcinoma of the breast based upon clinical examination MRI scan of the thorax would tend to show normal findings within the lungs and thorax.
Diagnosis
Diagnosis of Salmonella breast abscess / mastitis tends to be confirmed based upon bacteriology culture of aspiration specimens of the breast abscess and at times following pathology examination and microbiology culture of specimens of the breast lesion(s) that had been obtained by biopsy or mastectomy.
Treatment of patients who have Salmonella breast abscess / mastitis have included a combination of:
[1] The undertaking of Surgical treatment including:(a) complete aspiration of the breast which in a number of cases has been under ultrasound-scab guidance but in areas of the world where ultrasound scan facilities are not available by palpation to find the fluctuant lesion, (b) incision and drainage of the abscess (c) mastectomy (sub-cutaneous at times) when the lesion has been provisionally diagnosed of carcinoma of the breast and it is only after the results of the histopathology examination and bacteriology culture is obtained that the diagnosis of an abscess is made.
[2] Antibiotics – Utilization of correct antibiotic treatment based upon the sensitivity pattern of the cultured organism
Following utilization of aspiration or incision and drainage of the Salmonella breast abscess in combination with correct antibiotic treatment based upon the sensitivity pattern of the disease majority of the cases completely resolve.
Some of the differential diagnoses of Salmonella breast abscess include: Carcinoma of the breast, chronic inflammatory lesions of the breast / tuberculosis of the breast.
Al-Ishak et al [14]. reported the case of Salmonella enterica subsp enterica (1) serovar Enteritidis breast abscess in a 48-year-old woman who is a citizen of United Kingdom and who had travelled abroad. She was treated successfully with utilization of surgery and ciprofloxacin antibiotic treatment. Al-Ishak et al [14]. advised that unusual causative organisms should be borne in mind with regard to patients who had recently travelled abroad as well as pus should be sent for culture and sensitivity. They iterated that Mastitis that is caused by Salmonella spp. could manifest with a severely indurated area which could take a few weeks to resolve. They additionally stated that complete assessment biopsy of the indurated area as well as imaging of the breast is mandatory in order to exclude malignancy of the breast.
Brnčić et al [3]. reported a 70-year-old man who had manifested who was known to have non-insulin -dependent diabetes mellitus had manifested with a swelling with a swelling within his breast of 9 months duration. He did complain of minimal pain and he stated that the mass had grown slowly over the 9 months period. He was found on examination to have a 4 cm x 4 cm slightly painful left breast mass that was associated with livid discoloration of the overlying skin. His left breast nipple was noted to be retracted. He had mammography which demonstrated within his left retro-mammary pre-pectoral space, presence of two irregular, soft tissue density masses that contained microcalcifications as well as calcifications which did suggest the possibility of malignancy as a differential diagnosis as well as what was considered as the possibility of less likely diagnosis of a breast abscess. The level of his tumour marker CA 15.3 was noted to be normal at 8.7 with a reference range of 0.1 to 31.3 U/ML. He had diagnostic needle aspiration of about 20 millilitres of pus and cytological examination of the aspirated pus showed evidence of suppurative inflammation without any evidence of features of malignancy whilst awaiting the results of culture of the pus. He underwent left subcutaneous mastectomy and histopathology examination of the specimen showed chronic inflammation without any features of malignancy. Bacteriology culture of the pus showed a pure growth of Salmonella enterica serotype Enteritidis which was identified biochemically. The organism was sensitive to amoxicillin-clavulanic acid, ceftriaxone, trimethoprim-sulfamethoxazole, as well as ciprofloxacin. He was treated by means of oral medication of ciprofloxacin. Pursuant to the diagnosis of Salmonella breast abscess, the history of the patient was reviewed which did reveal a past history of an episode of severe acute gastro-entero-colitis 10 months earlier. A subsequent review of his medical history documentation did demonstrate that he had suffered from severe diarrhoea as well as vomiting which had lasted for 5 days with him becoming anuric 2 days preceding his admission into the Infectious Disease Department of one Regional Hospital. When he was admitted he was found to be severely dehydrated and he had signs of acute kidney failure and the results of his blood biochemistry test results were documented to include urea 40.4 millimoles / litre (reference range 2.8 to 8.3 millimoles / litre), and creatinine 824 millimoles / litre (normal range 79 to 125 millimoles / litre. He underwent haemodialysis five times which did result in his renal function. Salmonella Enteritidis was cultured from his stool specimen. He did not receive any antibiotic treatment. Some of the lessons that need to be learnt from this case report include the following: Even though breast abscess in a male is rare and breast abscess tends to be more commonly staphylococcal breast abscess, other breast abscesses could occur including: Salmonella breast abscess as well as tuberculous breast abscess and hence clinicians need to have a high index of suspicion for Salmonella breast abscess. Even though most common infections of the breast may manifest with pain, fever, swelling and acute inflammation of the breast, some cases of chronic inflammation of the breast may be due to Salmonella infection and tuberculous infection that may man0ifest with a lump/mass within the breast and minimal pain over a period many months whilst the patient may be well
Agrawal et al. [15] reported 2 cases of breast abscesses that were caused by salmonella enterica serotype para-typhi as follows:
Case 1
A 27-year-old lady presented painful lump within her left breast of 2 months duration. She reported that the lump started to grow bigger in size gradually over the preceding 2 months. She stated that the lump was in the first instance firm as well as painless, nevertheless, the lump did gradually grow in size and it became painful. She was not pregnant as well as she was not lactating at the time of her presentation. She was asymptomatic otherwise and she did not have any other co-morbidities. Her general and systematic examinations were within normal range. Clinical examination revealed that her left breast was tender and swollen. A mobile, soft, fluctuant mass that measured about 5 cm x 6 cm that was located within the lower quadrant of the left breast was found by palpation of her breast. The overlying skin of her left breast was noted to be warm as well as erythematous. No spontaneous discharge was observed from the abscess and there was no evidence of lymphadenopathy. The nipple was not retracted as well as there was no discharge from the nipple. Her axillary nodes were not palpable. She had ultrasound scan (USG) of her left breast which showed a heterogeneously hypo-echoic deep-seated irregular collection that measured about 4.9 cm x 3.5 cm. Based upon the features of her breast lesion, a diagnosis of breast abscess was made. The breast abscess was drained under ultrasound-scan-guidance and she was empirically commenced on amoxicillin-clavulanic acid 628 milligrams 8 hourly. The results of her laboratory tests showed a total leucocyte count of 12,500 / cubic millimetres, with 70% polymorphonuclear leucocytes. The aspirated pus was sent for microbiology examination. Ziehl-Neelsen staining of the pus did not demonstrate any evidence of acid fast bacilli (AFB) and GeneXpert test was negative for Mycobacterium tuberculosis. Gram staining of the pus did reveal numerous polymorphonuclear leucocytes as well as gram-negative bacilli. The culture of the pus grew cream-coloured non-haemolytic colonieson 5% sheep blood agar and non-lactose-fermenting colonies on MacConkey agar which were identified to be Salmonella enterica para-typhi A by means of matrix-assisted laser desorption ionization-time of flight mass spectrometry with utilization of the bioMérieux VITEK MS system (IVD data base version 2.0) (USA). The bacteria was found upon sensitivity testing to be sensitive to ciprofloxacin, trimethoprim-sulfamethoxazole, erythromycin, azithromycin, chloramphenicol, ceftazidime, ceftriazone, ampicillin as well as Nalidixic acid. As a result of the diagnosis, she was recalled and her past medical history was reviewed which revealed that she had gastroenteritis three months earlier which did resolve without any antibiotic treatment. Her stool, urine, and blood samples were obtained and submitted for culture but the results were negative for Salmonella para-typhi a spp. She had a Widal test which was found to be negative. She was subsequently treated with Azithromycin 1000 mg tablet once daily for five days. She responded well to treatment. Pursuant to ultrasound scan-guided aspiration of the pus and antibiotic treatment, she was cured and the abscess did not recur up to her one-year follow-up assessment.
Case 2
A 29-year-old lady did present with a lump within her left breast which she had developed over the preceding 20 days. She was not pregnant as well as she was not lactating at the time of her manifestation. Her breast examination revealed a lump that measured 4.5 cm x 3.5 cm within her left breast at 2 o’clock position that was free and not attached to the skin of her left breast as well as the underlying muscle. The skin overlying the breast lump appeared normal with no evidence of inflammation as well as no tenderness. The nipple was not retracted and there was no discharge from her nipple. There were no palpable axillary lymph nodes and the rest of her general examination as well as systemic examination were normal. A provisional diagnosis of breast lump that was suspicious for malignancy was made. She had routine blood tests and the results were normal. She had chest x-ray, ultrasound scan of both breasts, as well as core needle biopsy of both of her left breast lump. Ultrasound scan of her left breast showed heterogeneously hypo-echoic mass lesion that measured about 3.4 cm x 2.4 cm within her left breast at about 2 o’clock position. Pathology examination of the core needle biopsy of the left lump showed plenty of neutrophils as well as inflammatory cells that contained necrotic background suggestive of breast abscess. The lump was excised by means of radical duct excision. She was empirically treated by means of erythromycin 500 mg orally 6 hourly as well as metronidazole 400 mg twice daily for two weeks. The pus that was drained was sent for microbiology pathology examination. Gram staining of the drained pus demonstrated gram-negative bacilli. The culture on blood agar grew grey-white opaque, non-haemolytic colonies as well as non-lactose fermenting colonies on Mackonkey’s agar. The non-lactose fermenting gram negative bacillus was found to be Salmonella para-typhi A based upon mass spectrometry testing which was sensitive to the following antibiotics: Ciprofloxacin, trimethoprim-sulfamethoxazole, erythromycin, azithromycin, chloramphenicol, ceftazidime, and ceftriaxone, ampicillin, as well as nalidixic acid. She had blood culture and Widal test were undertaken and the results were negative. She received oral ciprofloxacin 500 mg twice per day for 14 days. She had ultrasound scan of her breast two weeks pursuant to two weeks of her antibiotic treatment which did not demonstrate any significant change in the heterogeneous hypo-echoic lesion. She underwent left breast lumpectomy with left radical milk duct excision. Some pus-like material that was obtained during the surgical procedure upon culture and sensitivity was found to have grown Salmonella para-typhi A that had similar anti-microbial sensitivity pattern. She received intravenous ceftriaxone 2 grams 12 hourly for seven days. Her follow-up assessment demonstrated complete resolution of the abscess.
On of abscess.
Some of the lessons learnt from these 2 cases include the following:
Baran et al [1]. reported a 43-year-old woman who presented with a lump, fever and mild pain in her breast. She was not pregnant or lactating at the time of her presentation. She did have a history of rheumatoid arthritis for 5 years and she was undergoing immunotherapy. She had ultrasound scan of her breast which demonstrated breast abscess. The abscess was drained and submitted for culture and sensitivity and Salmonella enterica serotype typhimurium was identified. The organism was sensitive to all of the anti0biotics that were tested. The patient was cured after surgical debridement and antibiotic therapy. The abscess did not recur pursuant to treatment. Baran et al [1]. presented the case to draw attention to non-typhoidal Salmonella an uncommon cause of breast abscess and they recommended the submission of specimens for bacteriological examination as well as treatment especially in cases of individuals who have underlying immunosuppressive diseases. Some of the lessons learnt from this summation include:
Viswanathan et al [16]. reported a 42-year-old married non-lactating lady who had noticed a swelling in her right breast about 15 days preceding her presentation in the hospital. She stated that she had high-grade fever and malaise preceding the swelling within her right breast. She also stated that she had noticed gradual increase in the size of her breast swelling that was associated with mild pain and no evidence of discharge from her nipple. She did not have any past history of breast disease. She did not have any history of loose motions, constipation or urinary abnormality and she had not received any TAB vaccination. She did not have any history of tuberculosis or contact with anyone who had tuberculosis. She did not have any menstrual irregularities as well as she was nulliparous, non-lactating at the time of her manifestation. She did not have any family history of any breast disease. She was found to be non-febrile, and her general and systematic examinations were normal. Her breast examination showed a single, firm, swelling that measured 5 cm x 6 cm x 5 cm within the upper outer quadrant of her right breast that was minimally tender, mobile, and non-adherent to the skin. The skin over the lump was normal but mildly dilated veins were visualised. The areola was normal and there was no discharge noticed from the nipple. Central group of her right axillary lymph nodes were palpable and her left breast did contain a small swelling that measured approximately 2 cm x 1 cm. Her left axilla was normal. No abnormality was found in her respiratory, alimentary, nervous as well as musculoskeletal systems. The differential diagnoses that were considered included chronic breast abscess and primary carcinoma of the breast. Diagnostic aspiration of the breast lesion was undertaken which was sent for culture and sensitivity. She was commenced on Amoxycillin and Clavulinic acid combination. Her haemoglobin level was 11.2 grams%, white blood cell count 7,500 (59% neutrophils). Culture and sensitivity of her aspirated pus from the breast grew a pure growth of Salmonella typhi which was sensitive to Ciprofloxacin, Ofloxacin, Norfloxacin, Ceftizomine, Cefuroxime, Ceftazidime, Cefaclor, Amikacin, Gentamycin, Netilmycin, Tobromycin, Piperacillin, Amoxycillin, Amoxycillin + Clavulinic acid, Ampicillin + Sulbactam, Cotrimoxazole, and Chloramphenicol. She had Widal test which revealed litres of Salmonella typhi H 1: 120, 0 1: 120. The titres of Salmonella para-typhi A and para-typhi B were nil. She had blood culture which did not yield any growth. Her urine and stool culture any pathogenic organism. The results of her biochemistry blood tests, Chest X-ray, and ECG were all normal. She had mammography which showed 2 cysts within her right breast that measured 2.4 cm x 1.9 cm each and a cyst in her left breast that measured 3.0 cm x 1.1 cm. She had ultrasound scan of her breasts which showed 2.1 cm x 1 cm and 3.5 cm x 1.2 cm cysts in her right breast and left breast respectively. She also had ultrasound of her abdomen which did not reveal any abnormality. She was treated conservatively by means of Ciprofloxacin 500 mg twice daily for 14 days and the size of cysts decreased and did not have any fever or systemic complaints. Repeat aspirations from the cysts were sent for culture which did not grow any organism. Upon subsequent examination, no further decrease in the size of the cyst was noted. The cyst was excised surgically. There was no growth in the culture of the specimen. Histopathology examination of the wall of the abscess demonstrated chronic inflammation.
Seah et al [17]. Reported a 7-week-old Chinese female who was admitted following her development of fever 1 day duration that was associated with 2 episodes of vomiting as well as reduced-feeding. She was found to have a furuncle of her right furuncle. She did not have any history of travelling or any relevant history of contact. No members of her family had diarrhoea. She did not consume any raw food or unpasteurized milk but was fed with expressed breast milk. There was a report of insufficient bottle hygiene in that her feeding bottle was rinsed only with hot water between expressed milk feeds. The results of her C-reactive protein (11.6 mg /DL) as well as her white blood cell count of 16.48 x 10 to the power 9 per litre were slightly raised. She had ultrasound scan of the breast which demonstrated a 0.5 cm x 0.5 cm abscess within her retro-areolar region. An aerobic blood culture was undertaken prior to the commencement of parenteral antibiotic treatment with ampicillin and cloxacillin which demonstrated a growth of Group C salmonella that was sensitive to ampicillin, ceftriaxone, and trimethoprim-sulfamethoxazole. Incision and drainage of the right breast abscess was undertaken on the 2nd day of her admission and culture of the specimen grew Group C Salmonella with the same antibiotic sensitivity pattern. Both isolates of the cultured organisms were typed to be Salmonella Mbandaka by Singapore National Public Health Laboratory. Her urine culture did not grow any organism. All her investigations were normal. Her pyrexia lysed on the 2nd day of her admission and a repeat blood culture was undertaken on the third day of her admission which did not grow any organism. Her antibiotic treatment was changed to ceftriaxone on the 4th day for clearance of possible biliary carriage of non-typhoidal Salmonella and also in order to ease her intramuscular administration of antibiotics due to her poor venous access. She initially developed mild diarrhoea of 5 loose stools on the 6th day of her admission. She was well and was discharged on the 9th day of her admission and completed 2 weeks of ceftriaxone which ensued by 1 week treatment of oral trimethoprim – sulfamethoxazole. Lessons learnt from this summation include:
Singh et al [9]. reported a case of bilateral breast abscesses that were caused by salmonella enterica serotype Typhi in a non-lactating 29-year old patient who had manifested with a lump in both breasts of 7 days duration. She also had intermittent discharge of pus-like substance from her nipples that was milky with regard to consistency. She also had fever of 1.5 months duration which was high-grade with a peak of 39.0 degrees centigrade which was brought down to normal range with antipyretics. She also did have loose episodes of loose motions over the preceding one month. She was commenced on co-amoxiclav (amoxycillin and clavulanic acid) 625 mg orally twice daily for 7 days but her symptom of pyrexia did not respond to the treatment. Her blood culture which was taken at home grew Salmonella Typhi which was resistant to amoxycillin but she did not attend to hospital to obtain a new medication. She was not pregnant and she was not lactating. Her clinical examination demonstrated a centrally located lump in her left breast that measured about 8 cm x 8 cm as well as another lump in her right breast that measured about 3 cm x 3 cm. Within her left axilla a palpable lump that measured 2 cm was found. Pus was drained from both breast lumps which on culture grew non-lactose fermenting colonies. The organism was identified as Salmonella Typhi which was sensitive to chloramphenicol, cefotaxime, ciprofloxacin, as well as cotrimoxazole, but which was also resistant to ampicillin and nalidixic acid. She also two weeks earlier had a report of Salmonella typhi positive culture 2 weeks preceding her manifestation that was sensitive to the same antibiotics. The result of her Widal tests was normal. The results of her routine haematology and biochemistry blood tests were within normal range with the exception of serum glutamic oxaloacetic transaminase (SGOT) and serum glutamic pyruvic transaminase (SGPT) which were raised with values of 96.59 and 113.78 U/L, respectively. She was commenced on oral ciprofloxacin 500 mg orally twice per day for 2 weeks to which she responded favourably with regression of the lesion. The results of her stool and urine culture were negative. Singh et al [9]. Made the ensuing conclusions:
Some of the lessons that need to be learnt from this summation include:
Murugesan et al [18]. reported a 60-year-old diabetic woman who was admitted because of fever over a period of 10 days which was ensued by pain and lump within her right breast for the preceding 2 days. She was afebrile and was found to have a lump that measured 7 cm by 5 cm within the upper outer quadrant of her right breast that was firm with regard to consistency and with no signs of inflammation. She had ultrasound scan of the breast which showed a right breast abscess which was subsequently treated by incision and drainage and the pus was submitted for culture and sensitivity. Salmonella typhi was cultured from the pus (see figure 1) that was sensitive to ampicillin-sulbactum as well as amikacin. His Widal test and blood culture were negative. He did completely recover completely with drainage of the abscess and antibiotic treatment.

Some of the lessons that had been learnt from this case report include:
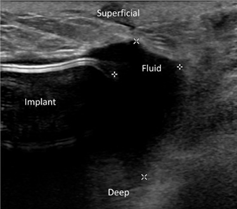
Hall et al [19]. reported the first case of traveller’s diarrhoea which had been ensued by breast implant infection. They reported an otherwise healthy 34-year-old woman, who had undergone breast augmentation with a left cremasteric lift (see figure 2). Five months pursuant to her breast operation, she was having a vacation in Cancun, Mexico, when she did develop abdominal pain as well as diarrhoea which had progressed to include fevers as well as chills. Her symptoms did persist until she returned to the United States of America. She was assessed by her primary care physician on the 4th day of her illness. He had computed tomography scan of her abdomen which did not demonstrate any abnormality. The results of her routine biochemistry blood tests did demonstrate raised levels of transaminase. Her symptoms did resolve soon. Fourteen days pursuant to the resolution of her symptoms, she did develop pain within her right breast (see figure 3). Upon examination her breast was found to be tender on palpation and swollen without any evidence of erythema. She had ultrasound scan of her breast which demonstrated a small amount of homogenous fluid encompassing her breast implant (see figures 4 and 5). She was prescribed Amoxicillin-Clavulanate 875-125 mg twice per day; nevertheless, she re-manifested three days later with worsening pain, swelling, as well as new erythema. She was taken to theatre where her breast abscess was drained with a total 200 MLS of purulent fluid and her breast implant was removed. Culture of her breast abscess grew Salmonella serogroup C. Based upon the sensitivity pattern of the cultured organism, her antibiotics was changed to sulfamethoxazole-trimethoprim 800-160 mg twice per day for 14 days and it was recommended that 4 additional months should pass before a new breast implant is inserted. Hall et al. [19] made the ensuing statements:



Deshpande et al [20]. reported a 35-year-old lady who had breast abscess that was caused by Salmonella Para-typhi A without any clinical evidence of having any enteric fever-like symptoms. The breast abscess case was managed with utilization of a combination antibiotic therapy and surgical option in order to treat the aetiological cause of the disease as well as the focal infection. Lessons that need to be learnt from this short summation include the following:
Brnčić et al [3]. reported a 70-year-old man who was known to have non-insulin dependent diabetes Mellitus, who had manifested with a swelling within his left breast over the preceding 9 months. He did complain of minimal pain in view of the fact that the mass had grown slowly over the 9 months period. His clinical examination demonstrated a 4 cm x 4 cm left breast mass that was slightly painful with livid discoloration of the overlying skin of the breast. The nipple of the left breast was also noted to be retracted. He had mammography which demonstrated within the left retro-mammary pre-pectoral space, presence of two irregular, soft-tissue density masses which had micro-calcifications as well as calcifications which was suggestive of a possible malignancy, or less likely a breast abscess. The result of his tumour marker CA 15-3, was found to be 8.7 U/ML, which was within the normal range of the laboratory of between 0.1 and 31.3 U/ML. Upon diagnostic aspiration of the left breast mass, 20 millilitres of pus was obtained and cytological examination of the pus whilst awaiting the results of the microbiology culture and sensitivity results demonstrated features of suppurative inflammation. He underwent sub-cutaneous mastectomy of his left breast and histopathology examination of the left breast specimen demonstrated features of chronic inflammation without any features to suggest the possibility of malignancy. Microbiology examination and culture of the pus showed a growth of Salmonella enterica serotype Enteritidis that was sensitive to Amoxicillin-Clavulanic acid, ceftriaxone, trimethoprim-sulfamethoxazole, as well as ciprofloxacin. He received ciprofloxacin oral medication. Pursuant to the establishment of Salmonella abscess of his left breast, his past medical history was reviewed and this revealed that he had developed an episode of severe diarrhoea and vomiting that lasted 5 days which was ensued by him developing anuria 2 days preceding his admission to the Infectious Diseases Department of one regional hospital. Upon his admission into the Infectious Diseases Department of the regional hospital, he was found to be severely dehydrated, with signs of acute renal failure, because of which he underwent haemodialysis 5 times that led to full recovery of his renal function. At that time Salmonella Enteritidis was isolated from his stool cultures. He did not receive any antibiotic treatment during this episode of Salmonella Enteritidis past infection. Some of the summating iterations made by Brnčić et al. [3] include the following:
Some of the lessons that need to be learnt from this case report include:
Sood [28] reported a 37-year-old lady who presented with fever on and off as well as pain within her right breast over the preceding 15 days. She had also noticed a lump within her right breast over the preceding 4 days. She had a one year history of type 2 diabetes mellitus with poor control of her glucose levels as well as a history of hypothyroidism. She was found to have a 4 cm x 4 cm lump within her right breast on the lateral outer quadrant as well as she had bilaterally mobile lymph nodes. She also had fever with a temperature of 101.7 degrees F. The results of all her routine haematology and biochemistry blood tests were normal with the exception of the fact that her serum thyroid stimulating hormone (TSH) level was raised at 6.15 micro IU/ML (normal range (0.2 to 4.20 micro IU/ML), and her fasting sugar (FBS) was raised at 130 MG/DL (normal range 74 to 99 MG/DL). She had bilateral mammograms which did not demonstrate any abnormality. She had ultrasound scan of her abdomen which demonstrated mild enlargement of liver with fatty infiltration of the liver. She had ultrasound scan of her breast and axilla which revealed well-defined heterogeneously defined hypo-echoic mass lesion that measured about 3.6 cm x 1.8 cm within her right breast which had involved the lateral aspect of the right breast. The dilated ducts did measure about 7-8 mm in calibre which showed thick echogenic material within it. The mammary ducts were seen to be covering towards the nipple. Many variable lymph nodes were seen in both axillary regions with the largest lymph node measuring 1.7 cm x 1.3 cm showing evidence of central necrosis. Ultrasound-guided fine needle aspiration cytology (FNAC) was undertaken and the examination of the specimen showed many neutrophils against a necrotic background that was suggestive of breast abscess. She underwent ultrasound scan-guided drainage of the breast abscess and the drained pus was sent for sent for culture and sensitivity and she was given intravenous Amikacin 500 mg 12 hourly plus Clindamycin 600 mg intravenously 12 hourly as well as Ofloxacin which she had been commenced on earlier was stopped.. The microbiology culture of the pus grew Salmonella Para-typhi A that was sensitive to Ceftriaxone, Chloramphenicol, Ampicillin, Tetracycline, Cotrimoxazole, Ciprofloxacin, as well as Ofloxacin but it was resistant to Nalidixic acid. Based upon the results of the pus culture sensitivity pattern, her treatment was changed to Ceftriaxone 2 grams intravenously 12 hourly. She had a WIDAL test and blood culture and both results were negative. She had a repeat ultrasound scan of her breast 3 days later and the scan did show thick pus within many dilated ducts in the lower outer quadrant of the breast with reactive lymph nodes. She underwent a repeat ultrasound-scan-guided aspiration drainage of the breast abscess and the pus which was sent for culture grew Salmonella Para-typhi A. She was discharged following 7 days of admission on Ceftriaxone 2 grams intravenously twice per day, Amikacin 250 mg intravenously twice per day, and capsule Dalacin (Clindamycin) 300 mg orally three times per day for 4 days and she was planned to be reviewed after 4 days. At her second follow-up 10 days after her discharge from hospital her abscess had completely resolved. A lesson learnt from this case report is that Salmonella breast abscess can be effectively treated by utilization of ultrasound scan-guided aspiration drainages and appropriate combination antibiotics based upon the sensitivity pattern of the cultured organism.
Singh et al [9]. reported a 29-year-old lady who had manifested with a lump within both of her breasts over the preceding 7 days that was associated with pain. The lumps were stated by her to be around her nipples and they were tender to touch with the overlying skin being warm. The pain was stated to be progressive in nature, sharp, as well as shooting pain. She had been having intermittent discharge of pus-like substance from her nipple which was milky with regard to its consistency. She did have high fever of 39 degrees centigrade over the preceding 1.5 months, which was improved by her intake of antipyretic medicament. She did have rare episodes of loose stools. Bowel motions over the preceding 1.5 months. Two weeks preceding the onset of her breast pain and breast lump, she did visit the medical out patients department of a hospital because of fever and she was empirically commenced on Amoxicillin-Clavulanic acid 625 mg twice per day for 7 days; nevertheless, her fever did not resolve. Although she did have blood culture which grew Salmonella typhi that was resistant to amoxicillin, she did not return for follow-up and she did not therefore, receive an appropriate antibiotic treatment based upon the sensitivity pattern of the cultured organism. She had two children but she was not pregnant and was not lactating. Her clinical examination demonstrated a centrally located lump within her left breast just underneath her areola that measured 3 cm x 3 cm. She was also found to have a palpable axillary lymph node that measured about 2 cm on the left side. She had drainage of pus from both of her breast lumps which upon culture grew Salmonella typhi in both cases that was sensitive to chloramphenicol, cefotaxime, ciprofloxacin, and co-trimoxazole, but which was resistant to Ampicillin and Nalidixic acid. She did have a positive blood culture of Salmonella typhi 2 weeks earlier which had a similar antibiotic sensitivity pattern. The result of her WIDAL test was negative and the result of her routine haematology and biochemistry blood tests were within normal range with the exception of her serum glutamine oxaloacetic transaminases (SGOT) as well as serum glutamine pyruvic transaminase (SGPT) that were raised at 96.59 and 113.78 U/L, respectively. She was commenced on oral ciprofloxacin 500 mg twice per day for 2 weeks and she did respond favourably with regression of the lesions. Her stool and urine cultures were negative for Salmonella typhi during her manifestation and subsequent follow-up visits. Singh et al [9]. Iterated the following:
Some of the lessons that need to be learnt from this case report include:
Singh et al [4]. reported a case of bilateral breast abscess due to Salmonella typhi in an unmarried 35-year-old woman, who did not have any predisposing conditions for the development of Salmonella breast abscess. She manifested with fever, and painful swelling of both of her breasts. Salmonella typhi was cultured from both of her breast abscesses. Singh et al [4]. stated that such uncommon cause of breast abscess should be suspected with regard to females who do not have any evidence of predisposing factors for the development of Salmonella breast abscess in order to provide effective treatment of the disease.
Hiyam et al [29]. reported an unusual case of recurrent bilateral breast abscess which had been caused by multiple organisms in an immunocompetent non-lactating patient. They reported that a 41-year-old non-diabetic Saudi single lady who had manifested in October 2015 with progressive left breast pain over the preceding 15 days that was associated with a lump within her left breast. She was found following thorough assessment to have a left breast abscess which was treated by means of intravenous antibiotics and incision and drainage of the breast abscess. Culture of the pus that was drained grew Pseudomonas aeruginosa (see table 1). Between October 2015 and January 2018 he required treatment for breast abscesses which had involved the breast which had involved the left breast alone, the right breast alone, or both breasts contemporaneously. In all including the first breast abscess the lady had developed breast abscesses on 10 different occasions between October 2015 and January 2018. The cultured bacteria did vary from one infection to the next and the organisms that were cultured would be summarised as follows: [1] October 2015 Left Breast -E Coli / Pseudomonas aeruginosa [2]. November 2015 Right and Left Breasts – E Coli / Proteus mirabilis [3]. January 2016 Right breast – E Coli / Pseudomonas aeruginosa [4] September 2016 Left Breast - E Coli / Proteus Mirabilis [5] September 2016 Right Breast -E Coli / Kocuria ristinae / Salmonella. [6] July 2017 - Right and Left Breast Mixed organisms [7]. July 2017 - Left and Right Breast -Proteus Mirabilis [8]. August 2017 - Left Breast -Proteus Mirabilis [9]. November 2017 - Right Breast - E Coli / Proteus Mirabilis, [10] January 2018 Right Breast - Klebsiella Pneumoniae / Citrobacter Species. She was investigated fully for the decrease in her appetite over the period between October 2015 and January 2018 and nothing was found except for positive Helicobacter Pylori stool antigen. Tests for hepatitis profile, HIV test, and tuberculosis (TB) test, were all negative as well as cancer screening test, IgG, IgM, IgE, were all normal. Anti endomyral antibodies were negative. Her breast biopsy was negative for cancer and for chronic inflammatory conditions [29].
A lesson that has been learnt from this case report is the fact that every pus that is drained from a breast abscess must be sent for culture and sensitivity including the primary breast abscess pus and all recurrent pusses that are drained because the causative organism and the antibiotic sensitivity pattern could be different. In the reported case there was a growth of Salmonella in one of the specimens contemporaneously with other bacteria.

Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
